Saint of the Day Quote: Saint Maximus of Naples
Bishop of Naples in the fourth century. Forced into exile, he was…


Bishop of Naples in the fourth century. Forced into exile, he was…

The first battle of the Civil War, Big Bethel was a classic…

This is why I support Trump even though he often irks me. …

God will send two punishments: one will be in the form of…

Massie, in all of his Jew hating glory, tried yesterday on…

Surrender? Surrender to whom, you bloody fool! They have no leader! Major…

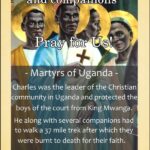
Firstly, that God’s church and all the Christian people of my dominions…

Could we at least have some dressing with the word salad?

News that I missed, courtesy of The Babylon Bee: SULLIVAN, ME —…

I’ve liked every Mormon I’ve met, but their theology has all the…
When Corpus Christi rolls around I always think of Saint Thomas…

If Liberation Theologians can make a bad faith case for the…

Charles the Great. He found the crown of the Roman…
Time is short. While we have it, let us do good. Saint…

Something for the weekend. FDR’s D-Day prayer. Bonus:

The men of the 5th Ranger Battalion could barely keep from…

Hard to believe that we are coming up on eighty-two years since…

Random observations on D-Day. Churchill and the King– Churchill had begun…

Our men simply could not get past the beach. They were pinned…

Concern about empathy is the entry drug for many ideas foreign…
My mission is to pray for the sanctification of families and…

“There is one great thing that you men will all be able…

The murderous parents received a fair amount of support on…

The Church is like a great ship being pounded by the waves…

If more vocations are wanted to the priesthood, make certain that…
Some additions: Sergeant York (1941) Joan of Arc (1948) Quo Vadis…
People who speak glibly today about a second civil war do…

In an instant the love of God was poured over me.…

The appointment of the head of EWTN News by Pope Leo…
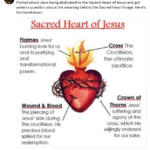
Do not be ashamed to confess the cross, for angels glory…

I am so old that I can recall when Popes did…
The late Bob Hope was justly famed for his entertainment of troops…

A generally good rule of life is to follow the advice you…

The usual Open Thread rules apply: be concise, be charitable and, above…
I am a Christian, and nothing vile is done…